Written By David Poulter – MSK Physiotherapist
A blog on the human intervertebral disc, movement, function, adaptation, degradation, degeneration, wedding photos, boiling frogs and Jelly Donut lies.
This blog is on all things about the human intervertebral disc and it’s beautiful structure which allows it to form multiple parts of the vertebral column primarily allowing motion of the protective column and transition of forces from the lower and upper limbs.
Firstly lets get some myths out of the way. Human discs do not slip, they really aren’t “discs”, they are nothing like a Jelly (jam) donut or a rubber washer, they do not exist in isolation and are made up of connective tissues of a predominantly cartilaginous nature. Thus their form is determined by their function and the ability of their cellular components to secrete extracellular material. They are living adaptable structures blending from the bone and endplate cartilage, they are intimately connected to both, forming a solid matrix joint allowing motion and load/force transfer. They work functionally in conjunction with their zygapophyseal joints to produce motion and stability to the vertebral column.
It is important to remember the lumbar discs are structurally different than the thoracic and cervical discs, they represent the classic annulus and nucleus seen in most text books. The cervical discs start out similar looking to lumbar discs but by the time we are adults they have remodelled into a more crescent shaped cartilaginous structure without a distinguishable annular nuclear arrangement as in the lumbar spine (1)

Fig: Section through a disc
Moving forward I will just focus on the lumbar intervertebral joint, and to be more precise the “interbody joint” which has colloquially become known as “the disc”.
The interbody joint is different from synovial joints and as a symphesis joint it has a solid construct with grading of it’s connective tissue structure based on the local joint internal forces and function. The outer capsule of the joint is the outer annulus which is fibrocartilagenous in nature,has a good vascular and nerve supply, like all joint capsules. The annulus is made up of fiberous collagen which has alternating angular fibers which producing a robust ligamentous structure that is ideal for resisting tensile forces. As you approach the inner joint the annulus blends into the nucleus which is high in Glycosaminoglycans (GAGs), hydrophilic (water attracting) in nature which give the nucleus (a slolid) the ability to resist compression and allows axial joint compression forces to be distributed to the annulus and endplate (2)
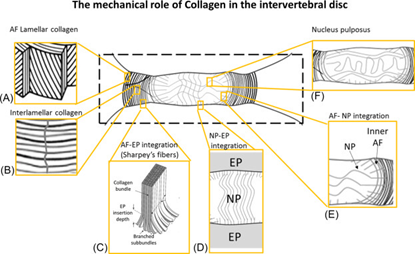
The Mechanical Role of Collagen Fibers in the Intervertebral Disc
The interbody joint (IV disc) is a living joint whose cells require nutrition to maintain homeostasis and the joints structure. The inner part of the joint (nucleus) is avascular and gets it’s nutrition from diffusion through the end plate and a small amount via the circulation of the outer annulus (3)
Thus movement, loading and then unloading of the joints are required to allow diffusion of oxygen and nutrients. The interbody joint, like all cartilage joint structures, requires movement and loading for life and health.
So to summarise the interbody joints are perfect for their function of load transfer and movement, they are one with the bones and endplate not separate enteties. They have a nerve supply and blood supply in they outer third and get their internal nutrition from diffusion. They are not rubber washers or anything like jelly donuts, they are a perfectly adapted hydraulic joint.
The interbody joints, due to their innervation, are a possible source of pain (nocicpetion) like all human joints. Much is written about the pathology that affect the joint from bulging, herniations to the dreaded “degenerative disc disease”, touted as a possible mechanism for chronic back pain. The problem is that degeneration of the interbody joint is common both in asymptomatic and symptomatic individuals (although there is a higher prevelance and correlation in people with symptoms in symptomatic people (4)
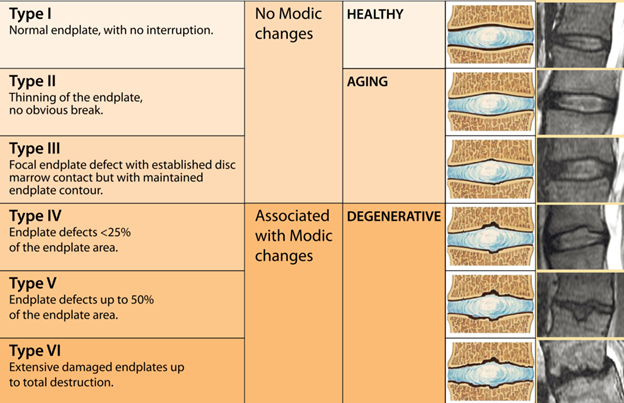
Degenerative changes tend to follow a regular course starting with degradation in the nucleus and progressing to the annulus (5)
The conundrum is that these changes are common in all age groups even adolescents (6) and their prevalence increase with age, but again are common in asymptomatic individuals (7)
So why do some people experience pain and others don’t?
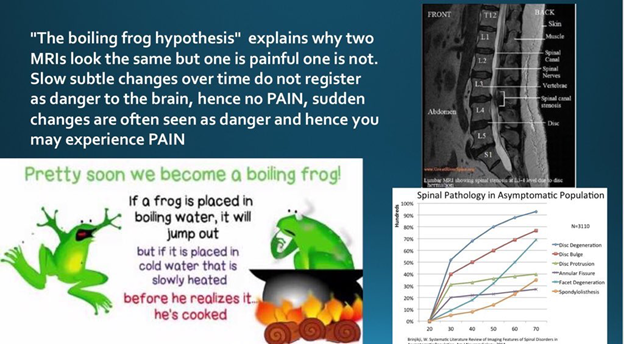
I propose the “Boiling Frog” hypothesis (see below)
I would also propose that the evidence for degenerative changes are that inherited genetics, occupational load exposure, sport exposure and lifestyle have moderate effect on the prevalence (8)
It is actually normal to have degenerative changes in the interbody joint as you age, it is also normal to have no symptoms. This would suggest that based on the Boiling Frog Hypothesis above , the changes seen on MRI scans in differing age groups are Normal Age (Activity) Related Adaptive Changes (NARAC) not a pathology or disease.
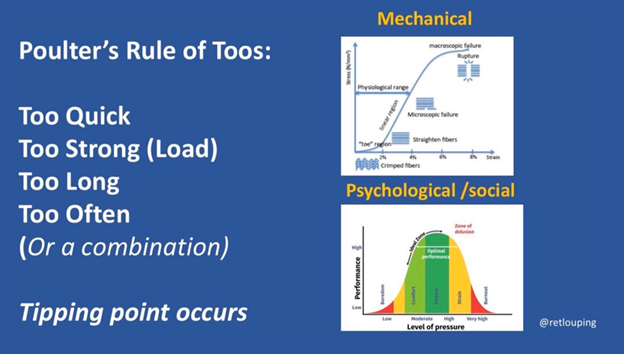
The reason that some people develop symptoms is probably also related to the rule of TOOs, both physical and psychosocial loads, as shown in the model below.
There inter-body joint can be strained and damaged under sudden or repetitive overload, like all joints in the human body. If the stress and load applied is within the capacity of the joint to remodel and adapt then no symptoms will ensue. There is evidence that the joint will adapt following Wolff’s law like most if not all connective tissue predominant structures (9)
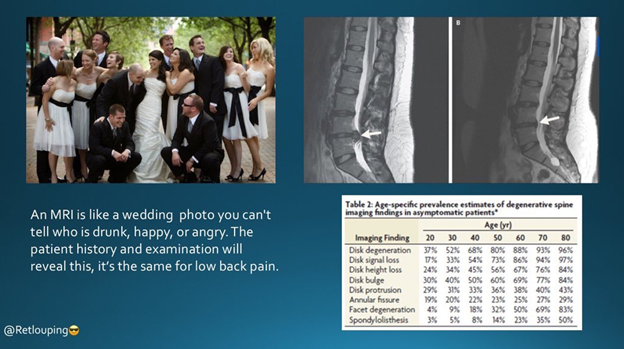
Degenerative changes on MRI may best be viewed as normal changes that develop over time than a disease or serious pathology. Due to the high incidence of so called “pathology” on the MRI scans of asymptomatic individuals I propose that the Wedding Photo model be used.
In conclusion, it may be normal to have degenerative changes on an MRI. There is some evidence that people with pain do have a higher incidence of degenerative findings, but we still do not know why. I propose that it is the development and mechanisms that produce the “pathology” on MRI which may lead to some people to develop symptoms whilst others don’t. Overloading the joint, which is innervated, may lead to a nociceptive event causing pain. The boiling frog model explains this, whilst using the wedding photo analogy will allow clinicians to rely on their patients history and examination not their scan results to formulate a diagnosis and treatment plan.
Beware of VOMIT Victims Of Modern Imaging Technology (10)
Remember degenerative changes are adaptation not pathology per se, MRIs can’t see pain, only the patients can report this.
Originally posted on https://www.physio-network.com/author/davidpoulter/?type=all
David Poulter
Recent Comments